2024: Volume 3, Issue 2
Current Issue
 Abstract
Abstract  PDF
PDFProtocol of the Percutaneous Tracheostomy Technique in a Porcine Model: Experimental Study
Guillermo Yanowsky Reyes1,3,4,6,7,*, Roberto Miguel Damián Negrete1,3,6, Mike Sepúlveda1, Juan Acosta1, Sergio Adrián Trujillo Ponce1,3, Eloy Sánchez Hernandez2, Rafael Santana Ortiz1, Jaime Orozco-Pérez1,3, Beda P Terrazas Moreno5, Arely Jaqueline Perez Padilla7
1Division of Pediatrics, Pediatric Surgery Service of the Guadalajara Civil Hospital “Fray Antonio Alcalde”, Guadalajara, Jalisco, Mexico
2Pediatric Anesthesiology Service, Guadalajara Civil Hospital “Fray Antonio Alcalde”, Guadalajara, Jalisco, Mexico
3Department of Human Reproduction, Child Growth and Development Clinics, University Center for Health Sciences, University of Guadalajara, Guadalajara, Jalisco, Mexico
4Lamar University, Health Sciences, Guadalajara, Jalisco, Mexico
5Division of Pediatrics, Western General Hospital, Guadalajara, Jalisco, Mexico
6Tlajomulco University Center University of Guadalajara, Mexico
7Tonalá University Center, University of Guadalajara, Mexico
*Corresponding author: Guillermo Yanowsky Reyes, Division of Pediatrics, Pediatric Surgery Service of the Guadalajara Civil Hospital “Fray Antonio Alcalde”, Guadalajara, Jalisco, Mexico, Phone: 3331572737, Email: [email protected]
Received Date: October 08, 2024
Publication Date: December 20, 2024
Citation: Reyes GY, et al. (2024). Protocol of the Percutaneous Tracheostomy Technique in a Porcine Model: Experimental Study. Gastro Res. 3(2):12.
Copyright: Reyes GY, et al. © (2024).
SUMMARY
Objective: To evaluate the applicability of the percutaneous tracheostomy placement technique guided by flexible bronchoscopy in a weaned or growing piglet model in order to know its reproducibility in pediatric patients considering their anatomical and weight similarity, and to describe a detailed technique in this group. Introduction: In the pediatric patient there is no detailed description of the technique, finding isolated reports in schoolchildren and adolescents, without a necessary equipment protocol individualized to each age group, emphasizing its scarce practice in children under 5 years of age, who can be benefited by this technique. Material and methods: Experimental study with 4 weaned porcine models of 5 weeks of age which were felt under the same systematized anesthetic protocol in which positioning technique was performed, adequate asepsis and antisepsis, diagnostic direct bronchoscopy during the performance of the endotracheal cannula placement technique monitoring early and late complications. Results: A total of 4 porcine models of male pigs weighing 5 kg were included in the study, which were submitted under anesthesia protocol prior to the performance of the tracheostomy placement technique by percutaneous puncture, so that 16 successful punctures were performed with the placement of 16 tracheostomy cannulas during the study. In each pig, 4 punctures were performed with 4 cannula insertions in the path of the cervical trachea, this technique was performed by 4 different prosecutors, each prosecutor performed the mentioned technique on 4 occasions successfully. The average time was 12 minutes with a range of 10 to 14 minutes. There were no complications or mortality associated with the technique. Discussion and conclusion: This paper describes the percutaneous tracheostomy placement technique and its reproducibility in pigs. The necessary material and the technique are shown in detail for an adequate application in clinical practice trying to resemble the pediatric patient. It can be concluded that the application of the technique in porcine models is successful, so its application in clinical practice in the pediatric patient can be considered. Considering the teaching and previous practice of the operator who carries out this procedure, knowing the risks and complications of it.
Keywords: Percutaneous Tracheostomy, Pigs, Pediatric Patients, Bronchoscopy, Technique
OBJECTIVE
To evaluate the applicability of the percutaneous tracheostomy placement technique guided by flexible bronchoscopy in a weaned or growing piglet model in order to know its reproducibility in pediatric patients considering their anatomical and weight similarity, and to describe a detailed technique in this group.
INTRODUCTION
The tracheostomy technique is defined as the surgical opening in the trachea, either as an open or percutaneous surgical procedure, usually performed between the 2nd and 4th tracheal ring, to maintain the airway patent and stable, useful in patients in critical that require prolonged mechanical ventilation, allows to prevent complications associated with orotracheal intubation such as pneumothorax, pneumomediastinum and airway injury, is more comfortable for the patient, improves hygiene bronchial and reduces the requirement for deep sedation [1,2].
The implementation of the tracheostomy was described in 1909 by Jackson, who describes the open technique, performing in operating rooms and with the disadvantage of the mobilization of the critical patient. In 1955 Shelden described for the first time the percutaneous tracheostomy with the passage of an arterial guide in a needle to channel the trachea but with multiple complications and high mortality rate. In 1985 Ciaglia used the Seldinger technique by means of serialized tracheal dilators through a mechanical guide. Until 1990 when Griggs described the last technique used together with Ciaglia with Rhino's blue graduated dilator [3].
The application of the technique depends on the operator with knowledge of the procedure, their training and experience being important. It is a minimally invasive tactic, simple because it requires few instruments, cheaper and faster because it does not require the use of the operating room and can be performed next to the patient's bed due to the low bleeding rate, without the need for potentially dangerous transfers compared to with conventional tracheostomy. It has favorable cosmetic results by leaving a smaller scar and decannulation with rapid closure of the stoma [1,2,4].
Early complications are serious, so adequate management, care and supervision are required during and after the procedure, among the most common are pneumothorax, subcutaneous emphysema, pneumomediastinum, false cannula tract, accidental decannulation and wound infection. Late complications in children range between 18.7 and 39%, with stomatal granulomas, accidental decannulation, cannula obstruction, and tracheal stenosis being the most reported. Reports indicate a mortality rate after tracheostomy in children from 0 to 18 years of age is 8%, being higher in children under 1 year of age [5].
In the pediatric patient there is no detailed description of the technique, finding isolated reports in schoolchildren and adolescents, without a necessary equipment protocol individualized to each age group, emphasizing its scarce practice in children under 5 years of age, who can benefit from this technique.
The proposal of this experimental model in weaned pig is made, with the objective of showing the practical application of percutaneous tracheostomy guided by flexible bronchoscopy, with the purpose of knowing its reproducibility in clinical practice by having resources and training of the same favoring Teaching it is considered viable due to its anatomical similarity to the pediatric patient [6-8].
Studio design
Experimental model in pig.
MATERIAL AND METHODS
An experimental model was carried out using four weaned male pigs of 5 weeks of age, which were subjected under a protocol of combined anesthesia with retroauricular peripheral route channeling with helmet No. 8, Hartman solution is administered at 20 m/kilo.
Two Stotz pediatric fiber endoscopes of 0.5 mm and 9 mm in diameter were used as a bronchoscopic guide at the time of puncture and for the verification of the introduction of the devices, 10 and 12 Fr dilator cannulas, Cook's 4 mm trichotomy set, benzol guides and walkers appropriate to the size and tracheal diameters of the pig. It had a set brand Cook, CPTI ®, Blue Rhino and Ultra-Perc ®.
Preparation measures
- Position decubito supino the pig.
- Orotracheal aspiration.
- Ventilation with ambient oxygen.
- Continuous monitoring of the pulse oximetry as a whole.
- Asepsis - antisepsis of the neck and chest.
- Position dorsal decubitus with neck extension.
- Placement of laryngeal mask No.1.
- Continuous ventilatory assistance.
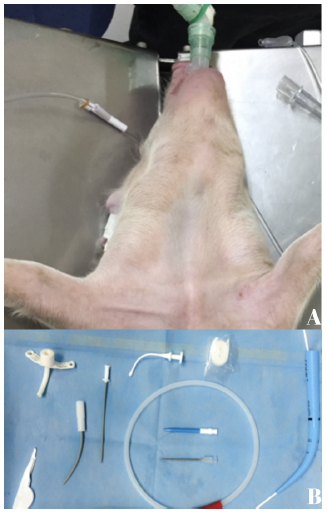
Figure 1. A) The pig model is shown. B) Material used during the percutaneous tracheostomy technique.
Sedation
- Rapid and short-acting sedation based on Pentobarbital at doses of 4 to 7 mg/kg/dose.
- Propofol-based maintenance sedation at doses of 3 to 6 ml/hour.
Required equipment
- Laryngeal mask No. 0.5 and 1.
- Laryngoscope.
- Endotracheal tubes.
- Vacuum cleaner.
- Feeding probes.
- Sterile / surgical gloves.
- Gauze.
- Cotton with alcohol.
- Disinfectant.
- Barren fields.
- Syringes.
- Hypodermic needles.
- Lidocaine
- TDP set.
- Tracheostomy cannula 3.5 mm ID.
- Lubricating jelly.
- Tape for fixing.
Procedure:
- A cannula is placed in the introducer by lubricating at one end, additional dilators are checked and lubricated.
- Diagnostic bronchoscopy is performed through a laryngeal mask to identify the anatomy of the pig, identifying the subglottic space and tracheal rings, direct vision continues during the procedure.
- Asepsis is performed - antisepsis, and the placement of sterile fields.
- Direct palpation is performed identifying the second tracheal ring.
- It infiltrates the space of the second tracheal ring
- Skin and soft tissue initiation is performed.
- Puncture is checked until the lumen of the airway is reached with the needle in the corresponding space by direct bronchoscopy.
- Control and take care of the collapse of the tracheal lumen (Physiological diameter of 0.8 to 1 mm)
- Check adequate puncture, absence of false pathway, that there is no subcutaneous emphysema.
- Passing seldinger guide without offering resistance up to 10 cm.
- Remove needle taking care of the seldinger guide.
- Pass the dilators gently by rotating motion.
- The Blue Rhino will be passed through the same technique with a smooth rotational movement.
- 3.5 mm ID endotracheal cannula is passed, verifying correct introduction without resistances, with adequate air passage, without subcutaneous emphysema, minimal bleeding and without evidence of tracheal collapse.
- The following was verified after the procedure:
Free passage of air through the light of the endotracheal cannula.
Symmetrical auscultation of both pulmonary fields.
Saturation in goals by pulse oximetry
16. After verifying the aforementioned, the cannula is fixed and a revision bronchoscopy is performed to conclude the procedure.
The tracheal diameter of the porcine model corresponds to that of a 1-year-old infant.
The estimated time of the procedure is 10 to 14 minutes.

Figure 2. A) Under diagnostic bronchoscopy, the subglottic space and tracheal rings are identified. B) Direct palpation is performed by identifying the second tracheal ring. C) Direct visualization by means of bronchoscopy of the placement of the cannula. D) Placement of endotracheal cannula 3.5 mm ID, verifying correct introduction without resistances, with adequate air passage.
RESULTS
A total of 4 porcine models of male pigs and technique for adequate application in clinical practice are shown in detail, trying to resemble the pediatric patient. The time required for percutaneous tracheostomy from sedation, placement, washing, puncture and final fixation in the model used was 12 minutes on average, similar to that reported by other authors. Likewise, we did not find early complications weighing 5 kg were included in the study, which were submitted under anesthesia protocol prior to the performance of the tracheostomy placement technique by percutaneous puncture, in such a way that 16 successful punctures were performed with the placement of 16 tracheostomy cannulas during the study. In each pig, 4 punctures were performed with 4 cannula insertions in the path of the cervical trachea, this technique was performed by 4 different prosecutors, each prosecutor performed the mentioned technique on 4 occasions successfully. The average time was 12 minutes with a range of 10 to 14 minutes. There were no complications or mortality associated with the technique.
DISCUSSION AND CONCLUSIONS
Tracheostomy is the surgical opening in the trachea that is made between the second and fourth tracheal ring, allowing patency of the airway. The most frequent indications for carrying it out are severe airway obstruction, prolonged mechanical ventilation and inadequate primitive reflexes [9]. The introduction of this procedure in the pediatric population is very promising due to its distinctive characteristics of feasibility to be carried out in any hospital environment with little material, being quick and with fewer short and long-term complications compared to the conventional technique. Although there are descriptions of the procedure in adolescent and adult patients, the technique is rarely described in children, which calls into question its reproducibility and results. This work describes the percutaneous tracheostomy placement technique and its reproducibility in pigs, an experimental animal model that is anatomically very similar to the study population. The necessary material such as bleeding or air leaks despite performing 4 placements in each pig [10,11].
It can be concluded that the application of percutaneous tracheostomy guided by flexible bronchoscopy in porcine models is safe and successful, so its application in clinical practice in pediatric patients can be considered, considering as the only limitation that teaching and prior practice of the operator performing this procedure. The technique described offers an alternative with greater benefits for the pediatric population, and can be considered and established as a first-line therapeutic approach [12].
ACKNOWLEDGMENTS
None.
DECLARATION OF CONFLICTS OF INTEREST
The authors declare that for this investigation no material or financial support was received that generates conflicts of interest.
REFERENCES
- Carboni Bisso I, Huespe I, Schverdfinger S, Videla C, Montagne J, Dietrich A, et al. (2020). Percutaneous tracheostomy guided by bronchoscopy: experience in 235 procedures. Revista de la Facultad de Ciencias Medicas (Cordoba, Argentina). 77(3):187-190.
- Gonzalez MG. (2009). Procedimiento de traqueostomía percutánea: control y seguimiento de enfermería. Enfermeria intensiva. 20(2):69-75.
- Johana Carolina Becerra Benitez Characterization of the tracheostomy in the intensive care unit of the San Rafael Clinical University Hospital in the period 2010 to 2013. (2014). New Granada Military University Bogotá.
- Andrés A, Rosario V, Jorge M, Paula O, Yuri Z, Julio Q, et al. Pediatric percutaneous trachestomy in ICU- Case report. (2016). Units of Otorhinolaryngology, Bronchopulmonary and Intensive Pediatrics Children's Hospital Roberto del Río. ISSSN: 0718-0918.
- Namavarian A, Levy BB, Tepsich M, McKinnon NK, Siu JM, Propst EJ, et al. (2024). Percutaneous tracheostomy in the pediatric population: A systematic review. Int J Pediatr Otorhinolaryngol. 177:111856.
- Balén EM, Sáez MJ, Cienfuegos JA, Zazpe CM, Ferrer JV, Herrera J, et al. (2000). Anatomy of the pig applied to experimentation in general surgery. Cirugía Española. 67:6.
- Bárbaraa SC, Rodríguez-Nunez A, López-Franco M, Martinón-Torres F, Martinón- Sánchez JM. (2005). Percutaneous tracheostomy under endoscopic control in adolescents. An Pediatr (Barc). 63(2):160-163.
- Gutiérrez-Núñez CA, Aguilera-González del Pino G, Fajardo-Pérez M. (2004). Percutaneous dilational tracheostomy. Description of the technique. Cuban Journal of Intensive Care Medicine and Emergencies. 3(4):124-134.
- Teresa MAG, Peco CB, Gordillo IL, Salido AG, Gaboli M. (2021). Tracheostomy and its care in pediatric patients. Pediatric Intensive Care Service. Niño Jesús Hospital, Madrid, Spain.
- Páez M, Buisán F, Almaraz A, Martínez- Martínez A, Muñoz, F. (2005). Percutaneous tracheotomy with the Ciaglia Blue Rhino® technique: A critical analysis after one year of experience. Spanish Journal of Anesthesiology Reanimation. 52:466-473.
- Paramio T, Manteca X, Milan J, Piedrafita J, Izquierdo MD, Gasa J, et al. Pig management and production. Brief manual of approach to the pig company for veterinary students. Departament de Ciència Animal i dels Aliments Unitat de Ciència Animal Facultat de Veterinària: UAB.
- Schweiger C, Manica D, Becker CF, Abreu LSP, Manzini M, Sekine L, et al. (2017). Tracheostomy in children: a ten-year experience from a tertiary center in southern Brazil. Brazilian Journal of Otorhinolaryngology. 83(6):627-632.