2024: Volume 3, Issue 2
Current Issue
 Abstract
Abstract  PDF
PDFOhmann Score versus Modified Alvarado Score for Diagnosis of Acute Appendicitis
Agrawal Srikant1,*, Maharjan Nayandra1, Bhusal Surendra2, Paudel Pratiksha3, Khatiwada Bidur4, Jha Rahul1, Shrestha Samrat1
1Department of General Surgery, Bir Hospital, National Academy of Medical Sciences(NAMS), Kathmandu, Nepal
2Department of Anesthesiology and Intensive Care, Bir Hospital, National Academy of Medical Sciences(NAMS), Kathmandu, Nepal
3Department of Internal Medicine, All Nepal Hospital, Kathmandu, Nepal
4Department of Internal Medicine, Nepalese Army Institute of Health Sciences, Kathmandu, Nepal
*Corresponding author: Dr. Srikant Agrawal, MS, Department of General Surgery, Bir Hospital, National Academy of Medical Sciences, Mahaboudha, Kathmandu 44600, Nepal, Tel: +9779860123448, ORCID: 0000-0002-0371-4821, Email: [email protected]
Received Date: September 16, 2024
Publication Date: October 11, 2024
Citation: Srikant A, et al. (2024). Ohmann Score versus Modified Alvarado Score for Diagnosis of Acute Appendicitis. Gastro Res. 3(2):11.
Copyright: Srikant A, et al. © (2024).
ABSTRACT Introduction: Acute appendicitis is one of the most common causes of acute abdomen. Early and accurate diagnosis is crucial to prevent morbidity and mortality. The Modified Alvarado Score is the most extensively used scoring system for diagnosing acute appendicitis. This study aims to assess the validity of the Ohmann Score in our population and compare it with the commonly used Modified Alvarado Score. Materials and Methods: A prospective comparative observational study was conducted in the Department of General Surgery at our hospital, enrolling a total of 85 patients with suspected acute appendicitis. The Ohmann Score and Modified Alvarado Score were calculated for each patient at the time of admission, and histopathological findings after surgery were correlated to predict the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for both scoring systems. Results: In this study, data from 85 patients were analyzed. The Modified Alvarado Score had a sensitivity of 59.49%, specificity of 66.67%, PPV of 95.92%, and NPV of 11.11%. In comparison, the Ohmann Score had a sensitivity of 89.87%, specificity of 83.33%, PPV of 98.61%, and NPV of 38.46%, demonstrating higher sensitivity, specificity, PPV, and NPV. The area under the ROC curve for the Ohmann Score was 0.866 (95% CI: 0.775–0.930), compared to 0.624 (95% CI: 0.513–0.727) for the Modified Alvarado Score. Conclusion: The Ohmann Score is a feasible and easy-to-use scoring system for diagnosing acute appendicitis, with better sensitivity, specificity, positive predictive value, and negative predictive value compared to the Modified Alvarado Score. Keywords: Acute Appendicitis, Ohmann Score, Modified Alvarado Score
INTRODUCTION
Acute inflammation of the vermiform appendix, a blind-ended tubular structure present at the convergence of the taenia coli arising from the cecum, denotes acute appendicitis [1]. It is one of the most common causes of acute abdomen, with a lifetime risk of developing the condition being 6.7% in females and 8.6% in males [2]. Early and accurate diagnosis is the cornerstone in the management of this condition to prevent morbidity and mortality [3,4]. Patients usually present with a sudden onset of pain in the peri-umbilical region, which then shifts to the right iliac fossa (RIF) and is associated with anorexia, nausea, vomiting, and fever. Tenderness and rebound tenderness elicited over the RIF is a vital clinical clue for its diagnosis. However, these typical findings are found in only 50–60% of cases, making early and accurate diagnosis of acute appendicitis challenging. Inaccurate diagnosis results in negative appendectomy rates ranging from 2-30%, whereas delayed surgical intervention can lead to perforation and peritonitis rates as high as 20% [2,3,5,6]. Imaging modalities like ultrasonography (USG), computed tomography (CT), and magnetic resonance imaging (MRI) have high sensitivity and specificity for the evaluation of patients with suspected acute appendicitis, but issues of availability, cost, and time raise questions about their application [2,5,7].
Given these diagnostic challenges, various scoring systems have been formulated for the accurate diagnosis of acute appendicitis. Alvarado proposed a scoring system in 1986 with a total score of 10 using eight parameters, including symptoms, signs, and laboratory variables, which was later modified by Kalan et al. in 1994 to create the Modified Alvarado Score (MAS) with a total score of 9. This has become the most extensively used scoring system today [8]. Similarly; Ohmann et al. developed the Ohmann Score in 1999 for the diagnosis of the same acute condition, taking into consideration the epidemiological aspects of the disease. The Ohmann Score includes age as a parameter, uses fewer laboratory parameters, and incorporates clinical variables, making clinical diagnosis more feasible [9].
In developing countries like ours, where there are resource constraints, a scoring system that includes fewer laboratory variables and has a higher diagnostic yield will help in the early and accurate diagnosis of acute appendicitis. This will ultimately reduce negative appendectomies, appendicular perforation peritonitis, morbidity, and mortality. This study is therefore conducted to assess the validity of the Ohmann Score in our population and to compare it with the extensively used Modified Alvarado Score.
MATERIALS AND METHODS Following the ethical clearance from the Institutional Review Board (IRB) of National Academy of Medical Sciences (NAMS), a prospective observational comparative study was conducted at Bir Hospital, Kathmandu, Nepal. Those patients who were admitted with diagnosis of acute appendicitis were included in the study excluding ones below 16 years, those managed conservatively, and those diagnosed as appendicular lump, abscess and perforation.
Sample size was calculated by using the formula:
n = {Z2 * Sensitivity (1 – sensitivity)} / (w2 * p)
Where,
n= sample size
Z = normal distribution value, set to 1.96 corresponding to 95% Confidence Interval
w = maximum acceptable width for 95% Confidence Interval set to 10%
p = prevalence
A detailed clinical history, clinical examination with appropriate investigations as per the hospital protocol was carried out by surgery postgraduate resident on duty at the emergency department and the data were recorded on a structured performa. Subsequently, the Ohmann and modified Alvarado scores were calculated. Cut-off values as suggested by the authors of these scores were taken for computation of sensitivity and specificity. On the basis of these scoring systems, the patients were divided into two groups; one as acute appendicitis and the other as other cause of acute abdomen. Final decision regarding management (operative, observation, discharge) of the case was made by surgeon on duty. Any surgical intervention was conducted by surgical team under the guidance and supervision of Consultant on duty. The intra-operative findings were recorded and retrieved specimens were sent for histological examination preserved in 10% Formalin. Intraoperative findings were documented as normal appendix, acute appendicitis, complicated appendicitis or other pathology.
The data collection was done on a separate proforma sheet for each patient. Data was collected till required number of sample was attained. The collected data was stored in an electronic database (MS-Excel Sheet) and statistical analyses were performed with statistical software (SPSS for Windows). Patients were stratified into different groups on the basis of cut off values suggested for each of Ohmann and modified Alvarado score and their sensitivity, specificity, positive predictive value and negative predictive value were calculated. Histopathological reports were taken as the reference for comparison. ROC curves were also obtained for these scores and area under the curves were compared for accuracy of the scores. A 95% confidence interval was taken, and p value less than 0.05 were considered as statistically significant.
RESULTS
The study was conducted with 85 patients suspected of acute appendicitis. The Ohmann score and Modified Alvarado score were calculated for each patient. The histopathological report was used as the reference for comparison, confirming 79 cases of acute appendicitis.
Table 1. Demographic data of patient diagnosed as acute appendicitis
|
Age(in years) |
Male |
Female |
Total |
|||
|
|
Number |
Percentage |
Number |
Percentage |
Number |
Percentage |
|
≤ 20 |
7 |
17.1 |
5 |
13.2 |
12 |
15.2 |
|
21-30 |
11 |
26.8 |
11 |
28.9 |
22 |
27.8 |
|
31-40 |
8 |
19.5 |
6 |
15.8 |
14 |
17.7 |
|
41-50 |
5 |
12.2 |
5 |
13.2 |
10 |
12.7 |
|
> 50 |
10 |
24.4 |
11 |
28.9 |
21 |
26.6 |
In this prospective study, the mean age of patients with acute appendicitis was found to be 37.87 years, with a standard deviation of ± 17.03.
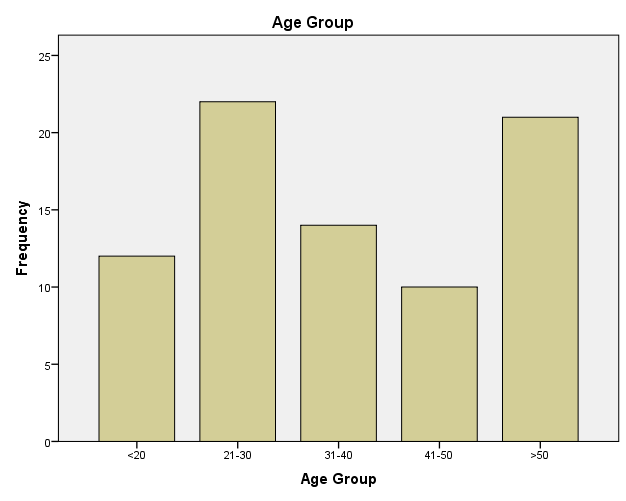
Figure 1. Age group distribution.
Similarly, the study found that the largest number of patients were in the age group 21-30 years, as shown in Table 1 and Figure 1.
Figure 2. Gender distribution.
Table 2. Presence of Symptoms in cases of Acute Appendicitis
|
Symptoms |
Number of Cases |
Percentage (%) |
|
Right iliac fossa pain |
|
|
|
Anorexia |
|
|
|
Nausea/ Vomiting |
|
|
|
Fever |
|
|
As shown in Table 2, the most common symptom was right iliac fossa pain. The majority of patients, 77 (97.5%), reported this symptom, while 65 (82.3%) experienced nausea and vomiting. Additionally, 47 (59.5%) patients developed anorexia, and the least number of patients, 13 (16.5%), complained of fever during history taking.
Table 3. Presence of signs in cases of Acute Appendicitis
|
Signs |
Number of Cases |
Percentage (%) |
|
Right iliac fossa tenderness |
79 |
100 |
|
Rebound tenderness Right iliac fossa |
70 |
88.6 |
Similarly, during clinical examination, 79(100%) patients had tenderness in the right iliac fossa while only 70 (88.6%) patients had signs of rebound tenderness in the right iliac fossa.
Table 4. Analysis of Ohmann score
|
Ohmann score |
Acute Appendicitis |
Not Acute Appendicitis |
Total (n-100) |
|
<6 |
|
|
|
|
6-11.5 |
|
|
|
|
≥ 12 |
|
|
|
|
Total (n) |
|
|
|
In this study, out of 72 patients with an Ohmann score of ≥12, 71 (98.6%) had histopathological examination (HPE) positive for appendicitis, while 1 (1.4%) had a negative HPE result. Similarly, out of 13 patients with an Ohmann score of 6–11.5, 8 (61.5%) had HPE-positive results, whereas 5 (38.5%) had HPE-negative results. Therefore, the study shows that the Ohmann score has a sensitivity of 89.87% (81.02% - 95.53%), specificity of 83.33% (35.88% -99.58%), positive predictive value (PPV) of 98.61% (92.21% - 99.77%), and negative predictive value (NPV) of 38.46% (22.83% - 56.91%).
Table 5. Analysis of modified Alvarado score
|
Modified Alvarado score |
Acute Appendicitis |
Not Acute Appendicitis |
Total (n-100) |
|
|
|
|
|
|
|
|
|
|
|
≥ 7 |
|
|
|
|
Total (n) |
|
|
|
Similarly, on analyzing the Modified Alvarado Score, out of 49 patients with an MAS score of ≥7, 47 (95.91%) had positive histopathological examination (HPE) results for appendicitis, while only 2 (4.08%) had negative HPE results. Out of 2 patients with an MAS score of 0-4, 1 (50%) had a positive HPE result and 1 (50%) had a negative HPE result. This analysis shows that the MAS scoring system has a sensitivity of 59.49% (47.85% - 70.40%), specificity of 66.67% (22.28% - 95.67%), positive predictive value (PPV) of 95.92% (88.19% - 98.67%), and negative predictive value (NPV) of 11.11% (6.27% - 18.94%).
Table 6. Comparison of Ohmann and modified Alvarado Scoring Systems
|
Index |
Ohmann score |
Modified Alvarado score |
|
Sensitivity (95% CI) |
89. 87% (81.02% - 95.53%) |
59.49% (47.85% - 70.40%) |
|
Specificity (95% CI) |
83.33% (35.88% - 99.58%) |
66.67% (22.28% - 95.67%) |
|
PPV (95% CI) |
98.61% (92.21% - 99.77%) |
95.92% (88.19% - 98.67%) |
|
NPV (95% CI) |
38.46% (22.83% - 56.91%) |
11.11% (6.27% - 18.94%) |
|
Accuracy (95% CI) |
89.41% (80.85% - 95.04%) |
60.00% (48.80% - 70.48%) |
|
p value |
< 0.001 |
|
|
ROC (95% CI) |
0.866 (0.775 – 0.930) |
0.624 (0.513 – 0.727) |
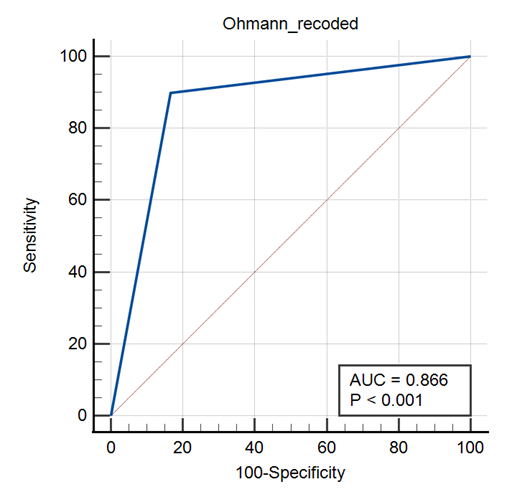
Figure 3. ROC of Ohmann Score.
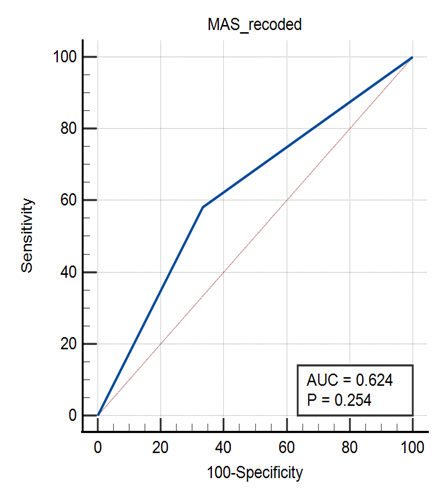
Figure 4. ROC of Modified Alvarado Score.
In this study, the area under the receiver operating characteristic (ROC) curve for the Ohmann score was 0.866 (95% CI; 0.775 – 0.930), while for the Modified Alvarado Score (MAS) it was 0.624 (95% CI; 0.513 – 0.727), as shown in Figures 3 and 4. The p-value for the Ohmann score was < 0.001, indicating statistical significance, whereas the p-value for the MAS was 0.254, indicating statistical insignificance, as detailed in Table 6.
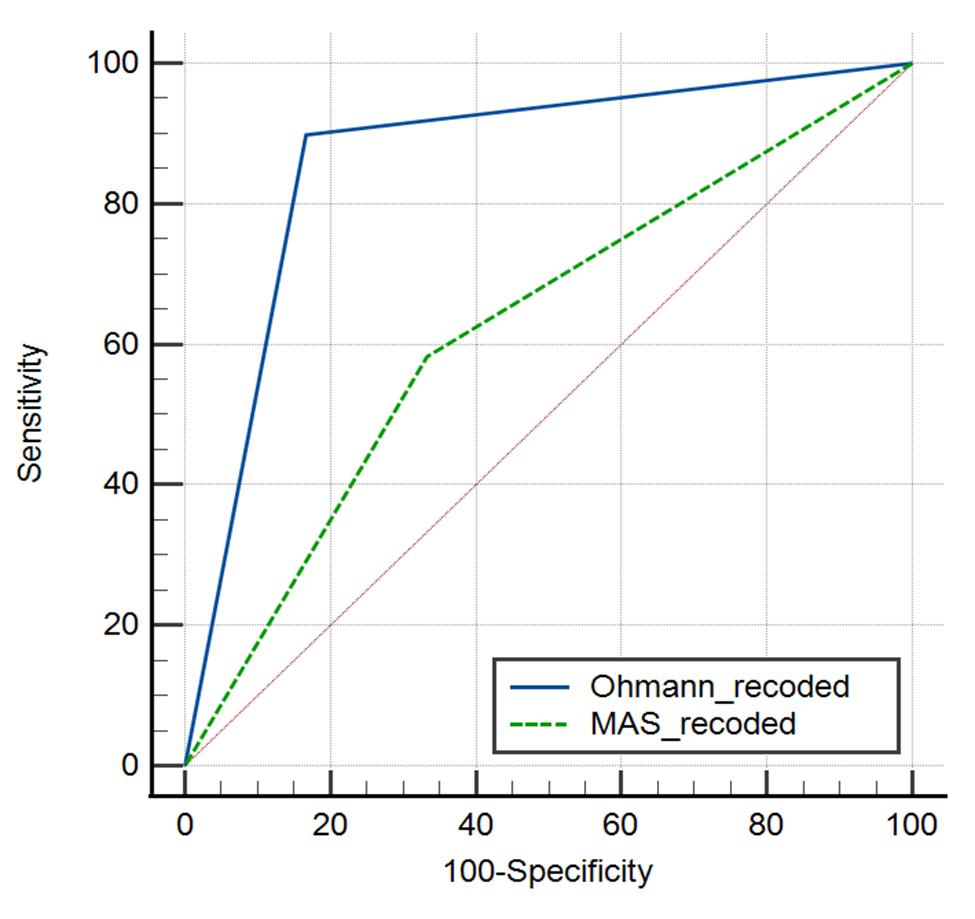
Figure 5. ROC of Ohmann score and Modified Alvarado Score.
On comparing the values of the Ohmann score with the Modified Alvarado Score (MAS), the p-value was 0.1231, indicating statistical insignificance (Figure 5).
DISCUSSION
Acute appendicitis is the most common surgical emergency worldwide [10,11]. Since its earliest description by Dr. Reginald Heber Fitz in 1886, establishing an early diagnosis has been a significant challenge in managing this condition. Delays in diagnosis can lead to delayed surgical intervention, resulting in higher morbidity and mortality [12]. Sophisticated diagnostic tools such as graded compression sonography, CECT abdomen, and diagnostic laparoscopy have proven effective, alongside various signs and symptoms, for diagnosing appendicitis [13]. Similarly, several scoring systems have been developed to aid in the early and accurate diagnosis of acute appendicitis [14]. These scoring systems each have their own sensitivity and specificity [15]. Among these, the Modified Alvarado Score and the Ohmann Score are commonly used [8,16]. Despite this, diagnosing acute appendicitis remains challenging due to the variable presentation of the disease and the lack of a reliable diagnostic test [17].
There are few studies comparing the Ohmann and Modified Alvarado scoring systems. Hence, this study prospectively compared these scoring systems by enrolling 85 patients suspected of acute appendicitis.
In this study, the highest number of acute appendicitis cases was found in the age group of 21-30 years, with a mean age of 37.87 ± 17.03 years. Similar results were found in studies by Talukdar et al., Chong et al., Deo et al., Jain et al., and Meltzer et al., where the most common age group was 21-30 years, and the mean age was approximately 31.57 ± 14. 14 and 35 years, which is close to our result [15,18-21]. The study also indicates that the incidence of acute appendicitis is higher in males than in females; out of 85 patients, 41 (51.9%) were male and 38 (48.1%) were female. A study on the epidemiology of acute appendicitis conducted in the United States, involving 250,000 patients, concluded that males had a higher incidence of appendicitis compared to females, with an overall ratio of 1.4:1. Similarly, Umar et al. (M= 1.5:1), Dahal et al., and Xingye et al. reported a higher prevalence in males compared to females (out of 84 patients, 65.4% were male and 34.5% were female) [11,22,23]. Additionally, Carditello A showed a male ratio of 3:1, and Ko Ys Lin Lh showed a ratio of 10:1 [24,25].
In this study, 77 (97.5%) patients had right iliac fossa pain, and 79 (100%) had tenderness over the right iliac fossa, indicating that the most common symptom is right iliac fossa pain and the most common sign is right iliac fossa tenderness. This is consistent with the study conducted by Ramchandra et al., where 87% of patients had right iliac fossa pain and 83% had tenderness over the RIF [26].
In the prospective study conducted by Kalan et al., the Modified Alvarado Score (MAS) of ≥7 showed a sensitivity of 100% in children, 93% in men, and 67% in women. Similarly, Umar et al. reported that MAS of ≥7 had sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy of 90.3%, 83.3%, 96.6%, 62.5%, and 89.2%, respectively. Jain et al. also found that MAS of 7-8 had a sensitivity of 86.1%, specificity of 83.3%, PPV of 98.9%, and NPV of 27.8% [8,21,22]. In contrast, in our study, MAS of ≥7 showed sensitivity of 59.49% (47.85% - 70.40%), specificity of 66.67% (22.28% - 95.67%), PPV of 95.92% (88.19% - 98.67%), and NPV of 11.11% (6.27% - 18.94%), which are lower compared to the aforementioned studies.
Ohmann et al. conducted a multicenter prospective interventional study in Germany and Austria, where an Ohmann score of ≥12 showed a sensitivity of 95.5%, specificity of 78.1%, PPV of 50.2%, and NPV of 98.7%.9 Similarly, Bharath et al. evaluated the Ohmann score and found that a score of ≥12 had an overall sensitivity of 75.5%, specificity of 78.5%, PPV of 94.33%, NPV of 40.74%, and diagnostic accuracy of 76.25% [27]. In our prospective study, an Ohmann score of ≥12 had sensitivity of 89.87% (81.02% - 95.53%), specificity of 83.33% (35.88% - 99.58%), PPV of 98.61% (92.21% - 99.77%), and NPV of 38.46% (22.83% - 56.91%), which are consistent with the results of previous studies. Therefore, the Ohmann score demonstrates higher sensitivity, specificity, PPV, and NPV compared to the MAS.
In our study, the area under the receiver operating characteristic (ROC) curve for the Ohmann score was 0.866 (95% CI; 0.688 – 1.000), while for the MAS it was 0.631 (95% CI; 0.402 – 0.859). Comparing the Ohmann score with the MAS, the p-value was 0.1231, indicating statistical insignificance. Similarly, in the study conducted by Hoseini et al., which compared the accuracy of the Ohmann and Alvarado scoring systems, the area under the ROC curve for the Ohmann score was 0.67 (95% CI; 0.598 to 0.742) and for the Alvarado score was 0.83 (95% CI; 0.77 – 0.88), with a p-value of 0.0001, indicating statistical significance [28].
CONCLUSION
Both the Ohmann Score and the Modified Alvarado Score are easy, fast, and reproducible scoring systems for the prompt diagnosis of acute appendicitis. However, imaging studies, combined with a high degree of clinical suspicion, are essential to reduce patient morbidity and mortality. This study shows that the Ohmann Score has higher sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) compared to the Modified Alvarado Score and is also comparatively easier to apply. Therefore, incorporating the Ohmann Score into daily practice for diagnosing acute appendicitis is feasible and justifiable. Nonetheless, similar studies with larger sample sizes and multi-institutional involvement are recommended.
LIMITATIONS
This study however has some limitations such as the sample size is relatively size and the exclusion of the paediatric population. Being a single institution based study narrows the possible implications of the findings in different setups. The effect of prior antimicrobial treatment from other health facilities was not addressed in this study.
ETHICAL CONSIDERATION
Ethical approval was obtained from the Institutional Review Board (IRB) of National Academy of Medical Sciences (NAMS), Kathmandu, Nepal.
DATA AVAILABILITY
The data supporting the findings of this study are available upon request from the corresponding author, Dr. Srikant Agrawal, MS. He can be contacted via email at [email protected]. Postal Address: Mahaboudha, Kathmandu 44600, Nepal.
FUNDING
None.
CONFLICT OF INTEREST
None.
PREVIOUS COMMUNICATION
This paper is not based on any previous communication to a society or meeting.
REFERENCES
- Mariadason JG, Wang WN, Wallack MK, Belmonte A, Matari H. (2012). Negative appendicectomy rate as a quality metric in the management of appendicitis: impact of computed tomography, Alvarado score and the definition of negative appendicectomy. Ann R Coll Surg Engl. 94(6):395-401.
- Malla BR, Batajoo H. (2014). Comparison of Tzanakis score vs Alvarado score in the effective diagnosis of acute appendicitis. Kathmandu Univ Med J (KUMJ). 12(45):48-50.
- Alvarado A. (2018). Diagnostic Scores in Acute Appendicitis [Internet]. Current Issues in the Diagnostics and Treatment of Acute Appendicitis. InTech. Available from: http://dx.doi.org/10.5772/intechopen.77230
- Addiss DG, Shaffer N, Fowler BS, Tauxe RV. (1990). The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 132(5):910-925.
- Gonullu E, Bayhan Z, Capoglu R, et al. (2022). Diagnostic Accuracy Rates of Appendicitis Scoring Systems for the Stratified Age Groups. Emerg Med Int. 2022:2505977.
- Al-Abed YA, Alobaid N, Myint F. (2015). Diagnostic markers in acute appendicitis. Am J Surg. 209(6):1043-1047.
- Mostbeck G, Adam EJ, Nielsen MB, et al. (2016). How to diagnose acute appendicitis: ultrasound first. Insights Imaging. 7(2):255-263.
- Kalan M, Talbot D, Cunliffe WJ, Rich AJ. (1994). Evaluation of the modified Alvarado score in the diagnosis of acute appendicitis: a prospective study. Ann R Coll Surg Engl. 76(6):418-419.
- Ohmann C, Franke C, Yang Q. (1999). Clinical benefit of a diagnostic score for appendicitis: results of a prospective interventional study. German Study Group of Acute Abdominal Pain. Arch Surg. 134(9):993-996.
- Omari AH, Khammash MR, Qasaimeh GR, Shammari AK, Yaseen MK, Hammori SK. (2014). Acute appendicitis in the elderly: risk factors for perforation. World J Emerg Surg. 9(1):6.
- Dahal I. (2022). Comparative Study of Modified Alvarado Score and Eskelinen Score in Diagnosing Acute Appendicitis. NMJ. 5(1):518-521.
- Streck CJ Jr, Maxwell PJ 4th. (2014). A brief history of appendicitis: familiar names and interesting patients. Am Surg. 80(2):105-108.
- Kirshtein B, Roy-Shapira A, Lantsberg L, Mandel S, Avinoach E, Mizrahi S. (2003). The use of laparoscopy in abdominal emergencies. Surg Endosc. 17(7):1118-1124.
- Alvarado A. (1986). A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 15(5):557-564.
- Meltzer AC, Baumann BM, Chen EH, Shofer FS, Mills AM. (2013). Poor sensitivity of a modified Alvarado score in adults with suspected appendicitis. Ann Emerg Med. 62(2):126-131.
- Khan I, ur Rehman A. (2005). Application of alvarado scoring system in diagnosis of acute appendicitis. J Ayub Med Coll Abbottabad. 17(3):41-44.
- Hlibczuk V, Dattaro JA, Jin Z, Falzon L, Brown MD. (2010). Diagnostic accuracy of noncontrast computed tomography for appendicitis in adults: a systematic review. Ann Emerg Med. 55(1):51-59.e1.
- DB T, Siddiq A. (2009). Modified Alvarado Scoring System. JAFMC Bangladesh. 5(1):18-20.
- Chong CF, Adi MI, Thien A, et al. (2010). Development of the RIPASA score: a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 51(3):220-225.
- Deo KK, Yogi P, Niroula A, Maharjan S. (2023). Appendicitis among Patients Admitted to the Department of Surgery of a Tertiary Care Centre: A Descriptive Cross-sectional Study. JNMA J Nepal Med Assoc. 61(257):10-13.
- Jain S, Gehlot A, Songra MC. (2018). Modified alvarado score in diagnosis of acute appendicitis: a clinicopathological study. Int Surg J. 5(3):878.
- Umar MM, Abubakar IU, Agbo SP. (2020). Comparative Study of Alvarado Score and its Modifications in the Preoperative Diagnosis of Acute Appendicitis at a Tertiary Center in Sokoto, Nigeria. Niger J Surg. 26(1):16-21.
- Xingye W, Yuqiang L, Rong W, Hongyu Z. (2018). Evaluation of Diagnostic Scores for Acute Appendicitis. J Coll Physicians Surg Pak. 28(2):110-114.
- Carditello A, Bartolotta M, Bonavita G, Lentini B, Sturniolo G. (1985). Appendicite acuta: considerazioni clinico-diagnostiche e terapeutiche [Acute appendicitis: clinico-diagnostic and therapeutic considerations]. Chir Ital. 37(2):174-182.
- Ko YS, Lin LH, Chen DF. (1995). Laboratory aid and ultrasonography in the diagnosis of appendicitis in children. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 36(6):415-419.
- J, Ramachandra & M, Sudhir & B.A, Sathyanarayana. (2013). EVALUATION OF MODIFIED ALVARADO SCORE IN PREOPERATIVE DIAGNOSIS OF ACUTE APPENDICITIS. Journal of Evolution of Medical and Dental sciences. 2(46):9019-9029.
- Sai Bharath N, Anurag M, Srinivas L, ganesh G. (2022). Evaluation of Ohmann Score in the Diagnosis of Acute Appendicitis in Patients Admitted in a Tertiary Care Hospital.European Journal of Molecular and Clinical Medicine. 9(3):4729+.
- Eshagh Hoseini SJ, Vahedian M, Sharifi A. (2021). Comparing the Accuracy of Ohmann and Alvarado Scoring Systems in Detection of Acute Appendicitis; a Cross-Sectional Study. Arch Acad Emerg Med. 9(1):e37.